Abstract
The system Urine Analyzer features new automatic checks for human urine. The analyzer automatically checks each test strip for humidity exposure, common sample interference and strip identification for any test strips. Together, these provide improved clinical information. Enhances confidence in clinical decisions with automatic checking performed on every test. Ensures consistent results interpretation with automatic timing and reading of every urine specimen
Ready for connectivity to data management solutions (DMS), via a simple matlab image processing. Offers a comprehensive point-of-care urinalysis menu for routine testing, detection of early kidney disease and hCG pregnancy testing

Introduction
Urine (from Latin Urina, ae, f.) is a liquid by-product of the body secreted by the kidneys through a process called urination and excreted through the urethra. Cellular metabolism generates numerous by-products, many rich in nitrogen, that require clearance from the bloodstream. These by-products are eventually expelled from the body during urination, the primary method for excreting water-soluble chemicals from the body. These chemicals can be detected and analyzed by urinalysis. Certain disease conditions can result in pathogen-contaminated urine.
Most animals have excretory systems for elimination of soluble toxic wastes. In humans, soluble wastes are excreted primarily by the urinary system and, to a lesser extent in terms of urea removed, by perspiration.[2]The urinary system consists of the kidneys, ureters, urinary bladder, and urethra. The system produces urine by a process of filtration, reabsorption, and tubular secretion. The kidneys extract the soluble wastes from the bloodstream, as well as excess water, sugars, and a variety of other compounds. The resulting urine contains high concentrations of urea and other substances, including toxins. Urine flows from the kidney through the ureter, bladder, and finally the urethra before passing from the body.
Exhaustive detailed description of the composition of human urine can be found in NASA Contractor Report No. NASA CR-1802, D. F. Putnam, July 1971.[3] That report provided detailed chemical analyses for inorganic and organic constituents, methods of analysis, chemical and physical properties and its behavior during concentrative processes such as evaporation, distillation and other physiochemical operations. Urine is an aqueous solution of greater than 95% water, with the remaining constituents, in order of decreasing concentration urea 9.3 g/L, chloride 1.87 g/L, sodium 1.17 g/L, potassium 0.750 g/L, creatinine 0.670 g/L and other dissolved ions, inorganic and organic compounds.
Urine is sterile until it reaches the urethra, where epithelial cells lining the urethra are colonized byfacultatively anaerobic Gram negative rods and cocci.[4] Current research suggests urine is not even sterile in the bladder.[5] Regardless, subsequent to elimination from the body, urine can acquire strong odors due to bacterial action,and in particular the release of ammonia from the breakdown of urea.
Some diseases alter the quantity and consistency of urine, such as diabetes introducing sugar. Consumingbeets can result in beeturia (pink/red urine containing betanin) for some 10–14% of the population.[6]
Most animals have excretory systems for elimination of soluble toxic wastes. In humans, soluble wastes are excreted primarily by the urinary system and, to a lesser extent in terms of urea removed, by perspiration.[2]The urinary system consists of the kidneys, ureters, urinary bladder, and urethra. The system produces urine by a process of filtration, reabsorption, and tubular secretion. The kidneys extract the soluble wastes from the bloodstream, as well as excess water, sugars, and a variety of other compounds. The resulting urine contains high concentrations of urea and other substances, including toxins. Urine flows from the kidney through the ureter, bladder, and finally the urethra before passing from the body.
Exhaustive detailed description of the composition of human urine can be found in NASA Contractor Report No. NASA CR-1802, D. F. Putnam, July 1971.[3] That report provided detailed chemical analyses for inorganic and organic constituents, methods of analysis, chemical and physical properties and its behavior during concentrative processes such as evaporation, distillation and other physiochemical operations. Urine is an aqueous solution of greater than 95% water, with the remaining constituents, in order of decreasing concentration urea 9.3 g/L, chloride 1.87 g/L, sodium 1.17 g/L, potassium 0.750 g/L, creatinine 0.670 g/L and other dissolved ions, inorganic and organic compounds.
Urine is sterile until it reaches the urethra, where epithelial cells lining the urethra are colonized byfacultatively anaerobic Gram negative rods and cocci.[4] Current research suggests urine is not even sterile in the bladder.[5] Regardless, subsequent to elimination from the body, urine can acquire strong odors due to bacterial action,and in particular the release of ammonia from the breakdown of urea.
Some diseases alter the quantity and consistency of urine, such as diabetes introducing sugar. Consumingbeets can result in beeturia (pink/red urine containing betanin) for some 10–14% of the population.[6]

characteristics of urine
Chemical analysis
Urine is principally water. It also contains an assortment of inorganic salts and organic compounds, including proteins, hormones, and a wide range of metabolites, varying by what is introduced into the body.
Color
Urine varies in appearance, depending principally upon a body's level of hydration, as well as other factors. Normal urine is a transparent solution ranging from colorless to amber but is usually a pale yellow. In the urine of a healthy individual the color comes primarily from the presence of urobilin. Urobilin in turn is a final waste product resulting from the breakdown of heme from hemoglobin during the destruction of aging blood cells.
Colorless urine indicates over-hydration, generally preferable to dehydration (though it can remove essential salts from the body). Colorless urine in drug tests can suggest an attempt to avoid detection of illicit drugs in the bloodstream through over-hydration.
Dark yellow urine is often indicative of dehydration.
Yellowing/light orange may be caused by removal of excess B vitamins from the bloodstream.
Certain medications such as rifampin and phenazopyridine can cause orange urine.
Bloody urine is termed hematuria, a symptom of a wide variety of medical conditions.
Dark orange to brown urine can be a symptom of jaundice, rhabdomyolysis, or Gilbert's syndrome.
Black or dark-colored urine is referred to as melanuria and may be caused by a melanoma.
Pinkish urine can result from the consumption of beets.
Greenish urine can result from the consumption of asparagus.
Reddish or brown urine may be caused by porphyria (not to be confused with the harmless, temporary pink or reddish tint caused by beeturia).
Blue urine can be caused by the ingestion of methylene blue (e.g., in medications).
Blue urine stains can be caused by blue diaper syndrome.
Purple urine may be due to purple urine bag syndrome.
Odor
The odor of normal human urine can reflect what has been consumed or specific diseases. For example, an individual with diabetes mellitus may present a sweetened urine odor. This can be due to kidney diseases as well, such as kidney stones.
Eating asparagus can cause a strong odor reminiscent of the vegetable caused by the body's breakdown of asparagusic acid.[8] Likewise consumption of saffron, alcohol, coffee, tuna fish, and onion can result in telltale scents. Particularly spicy foods can have a similar effect, as their compounds pass through the kidneys without being fully broken down before exiting the body.[9][10]
Turbidity
Turbid (cloudy) urine may be a symptom of a bacterial infection, but can also be caused by crystallization of salts such as calcium phosphate.
pH
The pH of urine can vary between 4.6 and 8, with neutral (7) being norm. In persons with hyperuricosuria, acidic urine can contribute to the formation of stones of uric acid in the kidneys, ureters, or bladder.[11] Urine pH can be monitored by a physician[12] or at home.
A diet high in citrus, vegetables, or dairy can increase urine pH (more basic).[13] Some drugs also can increase urine pH, including acetazolamide, potassium citrate, and sodium bicarbonate.
A diet high in meat can decrease urine pH (more acidic). Cranberries, popularly thought to decrease the pH of urine, have actually been shown not to acidify urine.[14] Drugs that can decrease urine pH include ammonium chloride, chlorothiazide diuretics, and methenamine mandelate.[15][16]
Volume
Average urine production in adult humans is about 1 – 2 L per day, depending on state of hydration, activity level, environmental factors, weight, and the individual's health. Producing too much or too little urine needs medical attention. Polyuria is a condition of excessive production of urine (> 2.5 L/day), oliguria when < 400 mL are produced, and anuria one of < 100 mL per day.
Density or specific gravity
Normal urine density or specific gravity values vary between 1.003–1.035 (g·cm−3), and any deviations may be associated with urinary disorders.
Urine is principally water. It also contains an assortment of inorganic salts and organic compounds, including proteins, hormones, and a wide range of metabolites, varying by what is introduced into the body.
Color
Urine varies in appearance, depending principally upon a body's level of hydration, as well as other factors. Normal urine is a transparent solution ranging from colorless to amber but is usually a pale yellow. In the urine of a healthy individual the color comes primarily from the presence of urobilin. Urobilin in turn is a final waste product resulting from the breakdown of heme from hemoglobin during the destruction of aging blood cells.
Colorless urine indicates over-hydration, generally preferable to dehydration (though it can remove essential salts from the body). Colorless urine in drug tests can suggest an attempt to avoid detection of illicit drugs in the bloodstream through over-hydration.
Dark yellow urine is often indicative of dehydration.
Yellowing/light orange may be caused by removal of excess B vitamins from the bloodstream.
Certain medications such as rifampin and phenazopyridine can cause orange urine.
Bloody urine is termed hematuria, a symptom of a wide variety of medical conditions.
Dark orange to brown urine can be a symptom of jaundice, rhabdomyolysis, or Gilbert's syndrome.
Black or dark-colored urine is referred to as melanuria and may be caused by a melanoma.
Pinkish urine can result from the consumption of beets.
Greenish urine can result from the consumption of asparagus.
Reddish or brown urine may be caused by porphyria (not to be confused with the harmless, temporary pink or reddish tint caused by beeturia).
Blue urine can be caused by the ingestion of methylene blue (e.g., in medications).
Blue urine stains can be caused by blue diaper syndrome.
Purple urine may be due to purple urine bag syndrome.
Odor
The odor of normal human urine can reflect what has been consumed or specific diseases. For example, an individual with diabetes mellitus may present a sweetened urine odor. This can be due to kidney diseases as well, such as kidney stones.
Eating asparagus can cause a strong odor reminiscent of the vegetable caused by the body's breakdown of asparagusic acid.[8] Likewise consumption of saffron, alcohol, coffee, tuna fish, and onion can result in telltale scents. Particularly spicy foods can have a similar effect, as their compounds pass through the kidneys without being fully broken down before exiting the body.[9][10]
Turbidity
Turbid (cloudy) urine may be a symptom of a bacterial infection, but can also be caused by crystallization of salts such as calcium phosphate.
pH
The pH of urine can vary between 4.6 and 8, with neutral (7) being norm. In persons with hyperuricosuria, acidic urine can contribute to the formation of stones of uric acid in the kidneys, ureters, or bladder.[11] Urine pH can be monitored by a physician[12] or at home.
A diet high in citrus, vegetables, or dairy can increase urine pH (more basic).[13] Some drugs also can increase urine pH, including acetazolamide, potassium citrate, and sodium bicarbonate.
A diet high in meat can decrease urine pH (more acidic). Cranberries, popularly thought to decrease the pH of urine, have actually been shown not to acidify urine.[14] Drugs that can decrease urine pH include ammonium chloride, chlorothiazide diuretics, and methenamine mandelate.[15][16]
Volume
Average urine production in adult humans is about 1 – 2 L per day, depending on state of hydration, activity level, environmental factors, weight, and the individual's health. Producing too much or too little urine needs medical attention. Polyuria is a condition of excessive production of urine (> 2.5 L/day), oliguria when < 400 mL are produced, and anuria one of < 100 mL per day.
Density or specific gravity
Normal urine density or specific gravity values vary between 1.003–1.035 (g·cm−3), and any deviations may be associated with urinary disorders.

Applications
Examination
Many physicians in ancient history have resorted to the inspection and examination of the urine of their patients. Hermogenes wrote about the color and other attributes of urine as indicators of certain diseases. Abdul Malik Ibn Habib of Andalusia d.862 AD, mentions numerous reports of urine examination throughout the Umayyad empire.[17] Diabetes mellitus got its name because the urine is plentiful and sweet. A urinalysis is a medical examination of the urine and part of routine examinations. A culture of the urine is performed when a urinary tract infection is suspected. A microscopic examination of the urine may be helpful to identify organic or inorganic substrates and help in the diagnosis.
The color and volume of urine can be reliable indicators of hydration level. Clear and copious urine is generally a sign of adequate hydration. Dark urine is a sign of dehydration. The exception occurs when diuretics or excessive amounts of alcohol or caffeine are consumed, in which case urine can be clear and copious and the person still be dehydrated.
Source of Medications
Urine contains proteins and other substances that are useful for medical therapy and are ingredients in many prescription drugs (e.g., Ureacin, Urecholine, Urowave). Urine from postmenopausal women is rich in gonadotropins that can yield follicle stimulating hormone and luteinizing hormone for fertility therapy.[18] One such commercial product is Pergonal.[19] Urine from pregnant women contains enough human chorionic gonadotropins for commercial extraction and purification to produce hCG medication. Pregnant mare urine is the source of estrogens, namely Premarin.[18] Urine also contains antibodies, which can be used in diagnostic antibody tests for a range of pathogens, including HIV-1.[20]
Other uses
Agriculture
Urine contains large quantities of nitrogen (mostly as urea), as well as significant quantities of dissolved phosphates and potassium, the main macronutrients required by plants, with urine having plant macronutrient percentages (i.e. NPK) of approximately 11-1-2 by one study[21] or 15-1-2 by another report,[22] illustrating that exact composition varies with diet. Undiluted, it can chemically burn the roots of some plants, but it can be used safely as a source of complementary nitrogen in carbon-rich compost.[23]
When diluted with water (at a 1:5 ratio for container-grown annual crops with fresh growing medium each season,[24] or a 1:8 ratio for more general use[23]), it can be applied directly to soil as a fertilizer. The fertilization effect of urine has been found to be comparable to that of commercial fertilizers with an equivalent NPK rating.[25] Urine contains most (94% according to Wolgast[21]) of the NPK nutrients excreted by the human body. Conversely, concentrations of heavy metals such as lead, mercury, and cadmium, commonly found in solid human waste, are much lower in urine (though not low enough to qualify for use in organic agriculture under current EU rules).[26] The more general limitations to using urine as fertilizer then depend mainly on the potential for buildup of excess nitrogen (due to the high ratio of that macronutrient),[24] and inorganic salts such as sodium chloride, which are also part of the wastes excreted by the renal system. The degree to which these factors impact the effectiveness depends on the term of use, salinity tolerance of the plant, soil composition, addition of other fertilizing compounds, and quantity of rainfall or other irrigation.
Urine typically contains 70% of the nitrogen and more than half the phosphorus and potassium found in urban waste water flows, while making up less than 1% of the overall volume. Thus far, source separation, or urine diversion and on-site treatment has been implemented in South Africa, China, and Sweden among other countries (with the Bill and Melinda Gates Foundation providing some of the funding for the implementations).[27] China reportedly had 685,000 operating source separation toilets spread out among 17 provinces in 2003.[28]
"Urine management" is a relatively new way to view closing the cycle of agricultural nutrient flows and reducing sewage treatment costs and ecological consequences such as eutrophication resulting from the influx of nutrient rich effluent into aquatic or marine ecosystems.[22] Proponents of urine as a natural source of agricultural fertilizer claim the risks to be negligible or acceptable. Their views seem to be backed by research showing there are more environmental problems when it is treated and disposed of compared with when it is used as a resource.[29]
It is unclear whether source separation, urine diversion, and on-site urine treatment can be made cost effective; nor whether required behavioral changes would be regarded as socially acceptable, as the largely successful trials performed in Sweden may not readily generalize to other industrialized societies.[25] In developing countries the use of whole raw sewage (night soil) has been common throughout history, yet the application of pure urine to crops is rare. Increasingly there are calls for urine's use as a fertilizer, such as a Scientific American article "Human urine is an effective fertilizer".[30]
Many physicians in ancient history have resorted to the inspection and examination of the urine of their patients. Hermogenes wrote about the color and other attributes of urine as indicators of certain diseases. Abdul Malik Ibn Habib of Andalusia d.862 AD, mentions numerous reports of urine examination throughout the Umayyad empire.[17] Diabetes mellitus got its name because the urine is plentiful and sweet. A urinalysis is a medical examination of the urine and part of routine examinations. A culture of the urine is performed when a urinary tract infection is suspected. A microscopic examination of the urine may be helpful to identify organic or inorganic substrates and help in the diagnosis.
The color and volume of urine can be reliable indicators of hydration level. Clear and copious urine is generally a sign of adequate hydration. Dark urine is a sign of dehydration. The exception occurs when diuretics or excessive amounts of alcohol or caffeine are consumed, in which case urine can be clear and copious and the person still be dehydrated.
Source of Medications
Urine contains proteins and other substances that are useful for medical therapy and are ingredients in many prescription drugs (e.g., Ureacin, Urecholine, Urowave). Urine from postmenopausal women is rich in gonadotropins that can yield follicle stimulating hormone and luteinizing hormone for fertility therapy.[18] One such commercial product is Pergonal.[19] Urine from pregnant women contains enough human chorionic gonadotropins for commercial extraction and purification to produce hCG medication. Pregnant mare urine is the source of estrogens, namely Premarin.[18] Urine also contains antibodies, which can be used in diagnostic antibody tests for a range of pathogens, including HIV-1.[20]
Other uses
Agriculture
Urine contains large quantities of nitrogen (mostly as urea), as well as significant quantities of dissolved phosphates and potassium, the main macronutrients required by plants, with urine having plant macronutrient percentages (i.e. NPK) of approximately 11-1-2 by one study[21] or 15-1-2 by another report,[22] illustrating that exact composition varies with diet. Undiluted, it can chemically burn the roots of some plants, but it can be used safely as a source of complementary nitrogen in carbon-rich compost.[23]
When diluted with water (at a 1:5 ratio for container-grown annual crops with fresh growing medium each season,[24] or a 1:8 ratio for more general use[23]), it can be applied directly to soil as a fertilizer. The fertilization effect of urine has been found to be comparable to that of commercial fertilizers with an equivalent NPK rating.[25] Urine contains most (94% according to Wolgast[21]) of the NPK nutrients excreted by the human body. Conversely, concentrations of heavy metals such as lead, mercury, and cadmium, commonly found in solid human waste, are much lower in urine (though not low enough to qualify for use in organic agriculture under current EU rules).[26] The more general limitations to using urine as fertilizer then depend mainly on the potential for buildup of excess nitrogen (due to the high ratio of that macronutrient),[24] and inorganic salts such as sodium chloride, which are also part of the wastes excreted by the renal system. The degree to which these factors impact the effectiveness depends on the term of use, salinity tolerance of the plant, soil composition, addition of other fertilizing compounds, and quantity of rainfall or other irrigation.
Urine typically contains 70% of the nitrogen and more than half the phosphorus and potassium found in urban waste water flows, while making up less than 1% of the overall volume. Thus far, source separation, or urine diversion and on-site treatment has been implemented in South Africa, China, and Sweden among other countries (with the Bill and Melinda Gates Foundation providing some of the funding for the implementations).[27] China reportedly had 685,000 operating source separation toilets spread out among 17 provinces in 2003.[28]
"Urine management" is a relatively new way to view closing the cycle of agricultural nutrient flows and reducing sewage treatment costs and ecological consequences such as eutrophication resulting from the influx of nutrient rich effluent into aquatic or marine ecosystems.[22] Proponents of urine as a natural source of agricultural fertilizer claim the risks to be negligible or acceptable. Their views seem to be backed by research showing there are more environmental problems when it is treated and disposed of compared with when it is used as a resource.[29]
It is unclear whether source separation, urine diversion, and on-site urine treatment can be made cost effective; nor whether required behavioral changes would be regarded as socially acceptable, as the largely successful trials performed in Sweden may not readily generalize to other industrialized societies.[25] In developing countries the use of whole raw sewage (night soil) has been common throughout history, yet the application of pure urine to crops is rare. Increasingly there are calls for urine's use as a fertilizer, such as a Scientific American article "Human urine is an effective fertilizer".[30]

Cleaning
Due to the fact that urea in urine breaks down into ammonia, urine has been used for the cleaning properties of the ammonia therein. In pre-industrial times urine was used – in the form of lant or aged urine – as a cleaning fluid.[31] Urine was also used for whitening teeth in Ancient Rome.
Due to the fact that urea in urine breaks down into ammonia, urine has been used for the cleaning properties of the ammonia therein. In pre-industrial times urine was used – in the form of lant or aged urine – as a cleaning fluid.[31] Urine was also used for whitening teeth in Ancient Rome.

Gunpowder
Urine was used before the development of a chemical industry in the manufacture of gunpowder. Urine, a nitrogen source, was used to moisten straw or other organic material, which was kept moist and allowed to rot for several months to over a year. The resulting salts were washed from the heap with water, which was evaporated to allow collection of crude saltpeter crystals, that were usually refined before being used in making gunpowder.[32]
Survival uses
The US Army Field Manual,[33] advises against drinking urine for survival. These guides explain that drinking urine tends to worsen, rather than relieve dehydration due to the salts in it, and that urine should not be consumed in a survival situation, even when there is no other fluid available. In hot weather survival situations where other sources of water are not available, soaking cloth (a shirt for example) in urine and putting it on the head can help cool the body.
During World War I the Germans experimented with numerous poisonous gases for use during war. After the first German chlorine gas attacks, Allied troops were supplied with masks of cotton pads that had been soaked in urine. It was believed that the ammonia in the pad neutralized the chlorine. These pads were held over the face until the soldiers could escape from the poisonous fumes, although it is now known that chlorine gas reacts with urine to produce toxic fumes (see chlorine and use of poison gas in World War I).The Vickers machine gun, used by the British Army during World War 1, required water for cooling when fired so soldiers would resort to urine if water was unavailable.[34]
Urban myth states that urine works well against jellyfish stings, and this scenario was demonstrated on a Season 4 episode of the NBC-TV show Friends called "The One With the Jellyfish"; an early episode of the CBS-TV show Survivor; The Paperboy (2012) wherein Nicole Kidman pees on Zac Efron's face; and the 2003 reality film The Real Cancun. However, at best it is ineffective, and in some cases this treatment may make the injury worse.[35][36][37]
Tanning
Tanners soaked animal skins in urine to remove hair fibers—a necessary step in the preparation of leather.
Textiles
Urine has often been used as a mordant to help prepare textiles, especially wool, for dyeing. In the Scottish Highlands and Hebrides, the process of "waulking" (fulling) woven wool is preceded by soaking in urine, preferably infantile.[38]
History and language
Prior to the acquisition of soap from the Germanic peoples during the first century AD, Ancient Romans used fermented human urine (in the form of lant) to cleanse grease stains from clothing.[39] The emperor Nero instituted a tax (Latin: vectigal urinae) on the urine industry, continued by his successor, Vespasian. It is Vespasian to whom the Latin saying Pecunia non olet (money doesn't smell) is attributed – said to have been the emperor's reply to a complaint from his son about the unpleasant nature of the tax. Vespasian's name is still attached to public urinals in France (vespasiennes), Italy (vespasiani), and Romania (vespasiene).
Alchemists spent much time trying to extract gold from urine, which led to discoveries such as white phosphorus by German alchemist Hennig Brand when distilling fermented urine in 1669. In 1773 the French chemist Hilaire Rouelle discovered the organic compound urea by boiling urine dry.
The onomatopoetic term "piss" was the usual word for urination prior to the 14th century. "Urinate" was at first used mostly in medical contexts. "Piss" continues to be used, but is considered vulgar; it is also used in such colloquialisms as "to piss off" and "piss poor". Euphemisms and expressions used between parents and children such as "wee", "pee", and many others, arose.
Aim of study
A urinalysis (UA), also known as routine and microscopy (R&M), is an array of tests performed on urine, and one of the most common methods of medical diagnosis.[1] The word is a portmanteau of the words urine and analysis.[2]
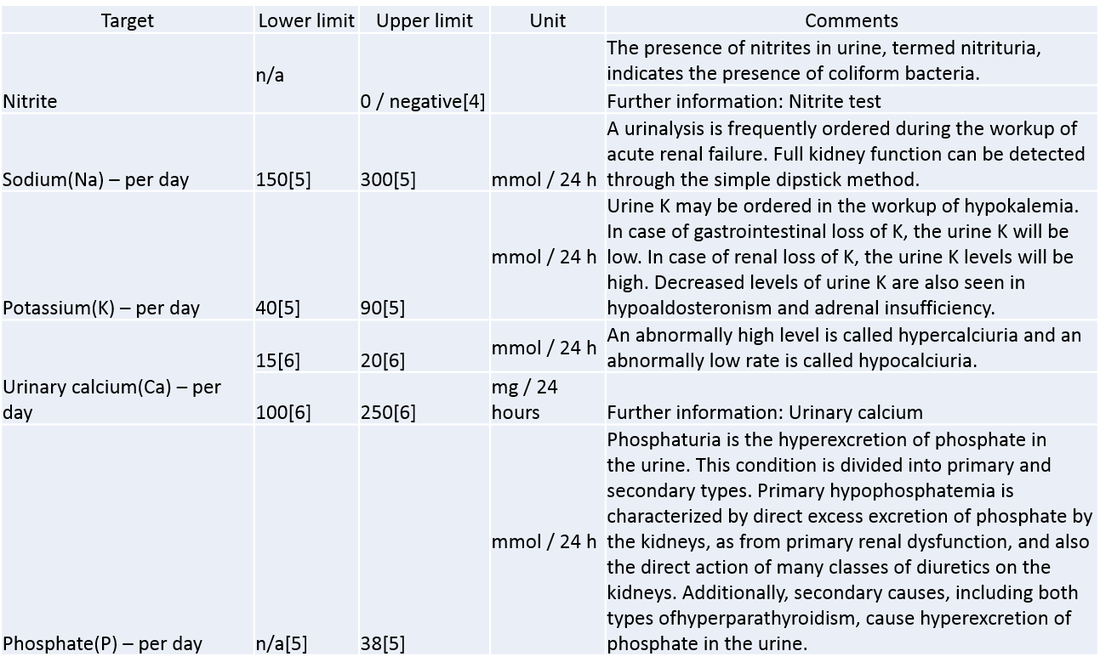
The target parameters that can be measured or quantified in urinalysis include many substances and cells, as well as other properties, such as specific gravity.
A part of a urinalysis can be performed by using urine test strips, in which the test results can be read as color changes. Another method is light microscopy of urine samples.
The target parameters that can be measured or quantified in urinalysis include many substances and cells, as well as other properties, such as specific gravity.
A part of a urinalysis can be performed by using urine test strips, in which the test results can be read as color changes. Another method is light microscopy of urine samples.

Methodology

Urine test strip
A urine test strip can quantify:
Leukocytes – with presence in urine known as leukocyturia
Nitrite – with presence in urine known as nitrituria
Protein – with presence in urine known as proteinuria, albuminuria, or microalbuminuria
Blood – with presence in urine known as hematuria
specific gravity
Microscopic examination
A urine sample is about to be examined under a phase-contrast microscope using a Neubauer counting chamber. The urine is under the cover slide, in the upper segment formed by the H-shaped grooves.
The numbers and types of cells and/or material such as urinary casts can yield a great detail of information and may suggest a specific diagnosis.
Hematuria – associated with kidney stones, infections, tumors and other conditions
Pyuria – associated with urinary infections
Eosinophiluria – associated with allergic interstitial nephritis, atheroembolic disease
Red blood cell casts – associated with glomerulonephritis, vasculitis, or malignant hypertension
White blood cell casts – associated with acute interstitial nephritis, exudative glomerulonephritis, or severe pyelonephritis
(Heme) granular casts – associated with acute tubular necrosis
Crystalluria – associated with acute urate nephropathy (or acute uric acid nephropathy, AUAN)
Calcium oxalatin – associated with ethylene glycol
Waxy casts – associated with chronic renal disease
Other methods of urinalysis
Urine culture – a microbiological culture of urine samples, detecting bacteriuria, is indicated when a urinary tract infection is suspected.
Ictotest – this test is used to detect the destruction of old red blood cells in the urine.
Hemoglobin test – this tests for hemolysis in the blood vessels, a rupture in the capillaries of the glomerulus, or hemorrhage in the urinary system, which cause hemoglobin to appear in the urine.
A urine test strip can quantify:
Leukocytes – with presence in urine known as leukocyturia
Nitrite – with presence in urine known as nitrituria
Protein – with presence in urine known as proteinuria, albuminuria, or microalbuminuria
Blood – with presence in urine known as hematuria
specific gravity
Microscopic examination
A urine sample is about to be examined under a phase-contrast microscope using a Neubauer counting chamber. The urine is under the cover slide, in the upper segment formed by the H-shaped grooves.
The numbers and types of cells and/or material such as urinary casts can yield a great detail of information and may suggest a specific diagnosis.
Hematuria – associated with kidney stones, infections, tumors and other conditions
Pyuria – associated with urinary infections
Eosinophiluria – associated with allergic interstitial nephritis, atheroembolic disease
Red blood cell casts – associated with glomerulonephritis, vasculitis, or malignant hypertension
White blood cell casts – associated with acute interstitial nephritis, exudative glomerulonephritis, or severe pyelonephritis
(Heme) granular casts – associated with acute tubular necrosis
Crystalluria – associated with acute urate nephropathy (or acute uric acid nephropathy, AUAN)
Calcium oxalatin – associated with ethylene glycol
Waxy casts – associated with chronic renal disease
Other methods of urinalysis
Urine culture – a microbiological culture of urine samples, detecting bacteriuria, is indicated when a urinary tract infection is suspected.
Ictotest – this test is used to detect the destruction of old red blood cells in the urine.
Hemoglobin test – this tests for hemolysis in the blood vessels, a rupture in the capillaries of the glomerulus, or hemorrhage in the urinary system, which cause hemoglobin to appear in the urine.
Literature Review (click on material to open actual papers)
Background: DD3PCA3 is the most prostate cancer-specific gene described to date. To assess the clinical utility of DD3PCA3 a time-resolved fluorescence-based, quantitative RT-PCR analysis for DD3PCA3 was developed.
Methods: The diagnostic potential of DD3PCA3 was determined by quantitative measurement of DD3PCA3 transcripts in non-malignant and malignant prostate specimens. Moreover, DD3PCA3 transcripts were determined quantitatively in urine sediments obtained after prostatic massage. A cohort of 108 men, admitted for prostate biopsies based on a PSA of >3 ng/ml, was studied.
Results: Prostate tumors showed a 66-fold up-regulation of DD3PCA3 (median 158.4·105 copies/μg tissue RNA) when compared to benign prostate tissue (median 2.4·105 copies/μg tissue RNA). This up-regulation was found in more than 95% of prostate cancer specimens studied. These data revealed that specimens with less than 10% of cancer cells could be accurately discriminated from non-cancer tissues. Hence, detection of a small fraction of prostate cancer cells in a background of normal cells seemed feasible. Therefore, this DD3PCA3-based RT-PCR assay was used for the identification of prostate cancer in urine sediments obtained after prostatic massage. From 108 men with a serum PSA value >3 ng/ml, 24 men were shown to have prostate cancer upon biopsy. Of these 24 men, 16 were shown to be positive for DD3PCA3, indicating a sensitivity of the assay of 67%. Furthermore, a negative predictive value of 90% was calculated.
Conclusion: The quantitative RT-PCR assay for DD3PCA3 described, bears great promise as a tool for molecular urine analysis. It has great potential in reducing the number of unnecessary biopsies. A multi-center study using this DD3PCA3 assay can provide the basis for the utility of molecular diagnostics in clinical urological practice.
Methods: The diagnostic potential of DD3PCA3 was determined by quantitative measurement of DD3PCA3 transcripts in non-malignant and malignant prostate specimens. Moreover, DD3PCA3 transcripts were determined quantitatively in urine sediments obtained after prostatic massage. A cohort of 108 men, admitted for prostate biopsies based on a PSA of >3 ng/ml, was studied.
Results: Prostate tumors showed a 66-fold up-regulation of DD3PCA3 (median 158.4·105 copies/μg tissue RNA) when compared to benign prostate tissue (median 2.4·105 copies/μg tissue RNA). This up-regulation was found in more than 95% of prostate cancer specimens studied. These data revealed that specimens with less than 10% of cancer cells could be accurately discriminated from non-cancer tissues. Hence, detection of a small fraction of prostate cancer cells in a background of normal cells seemed feasible. Therefore, this DD3PCA3-based RT-PCR assay was used for the identification of prostate cancer in urine sediments obtained after prostatic massage. From 108 men with a serum PSA value >3 ng/ml, 24 men were shown to have prostate cancer upon biopsy. Of these 24 men, 16 were shown to be positive for DD3PCA3, indicating a sensitivity of the assay of 67%. Furthermore, a negative predictive value of 90% was calculated.
Conclusion: The quantitative RT-PCR assay for DD3PCA3 described, bears great promise as a tool for molecular urine analysis. It has great potential in reducing the number of unnecessary biopsies. A multi-center study using this DD3PCA3 assay can provide the basis for the utility of molecular diagnostics in clinical urological practice.
Background
Positron emission tomography (PET) studies of major depression have revealed resting-state abnormalities in the prefrontal and cingulate cortices. Recently, fMRI has been adapted to examine connectivity within a specific resting-state neural network—the default-mode network—that includes medial prefrontal and anterior cingulate cortices. The goal of this study was to examine resting-state, default-mode network functional connectivity in subjects with major depression and in healthy controls.
Methods
Twenty-eight subjects with major depression and 20 healthy controls underwent 5-min fMRI scans while resting quietly. Independent component analysis was used to isolate the default-mode network in each subject. Group maps of the default-mode network were compared. A within-group analysis was performed in the depressed group to explore effects of depression refractoriness on functional connectivity.
Results
Resting-state subgenual cingulate and thalamic functional connectivity with the default-mode network were significantly greater in the depressed subjects. Within the depressed group, the length of the current depressive episode correlated positively with functional connectivity in the subgenual cingulate.
Conclusions
This is the first study to explore default-mode functional connectivity in major depression. The findings provide cross-modality confirmation of PET studies demonstrating increased thalamic and subgenual cingulate activity in major depression. Further, the within-subject connectivity analysis employed here brings these previously isolated regions of hypermetabolism into the context of a disordered neural network. The correlation between refractoriness and subgenual cingulate functional connectivity within the network suggests that a quantitative, resting-state fMRI measure could be used to guide therapy in individual subjects.
Positron emission tomography (PET) studies of major depression have revealed resting-state abnormalities in the prefrontal and cingulate cortices. Recently, fMRI has been adapted to examine connectivity within a specific resting-state neural network—the default-mode network—that includes medial prefrontal and anterior cingulate cortices. The goal of this study was to examine resting-state, default-mode network functional connectivity in subjects with major depression and in healthy controls.
Methods
Twenty-eight subjects with major depression and 20 healthy controls underwent 5-min fMRI scans while resting quietly. Independent component analysis was used to isolate the default-mode network in each subject. Group maps of the default-mode network were compared. A within-group analysis was performed in the depressed group to explore effects of depression refractoriness on functional connectivity.
Results
Resting-state subgenual cingulate and thalamic functional connectivity with the default-mode network were significantly greater in the depressed subjects. Within the depressed group, the length of the current depressive episode correlated positively with functional connectivity in the subgenual cingulate.
Conclusions
This is the first study to explore default-mode functional connectivity in major depression. The findings provide cross-modality confirmation of PET studies demonstrating increased thalamic and subgenual cingulate activity in major depression. Further, the within-subject connectivity analysis employed here brings these previously isolated regions of hypermetabolism into the context of a disordered neural network. The correlation between refractoriness and subgenual cingulate functional connectivity within the network suggests that a quantitative, resting-state fMRI measure could be used to guide therapy in individual subjects.
Physiology of urine
Introduction
The Urinary System is a group of organs in the body concerned with filtering out excess fluid and other substances from the bloodstream. The substances are filtered out from the body in the form of urine. Urine is a liquid produced by the kidneys, collected in the bladder and excreted through the urethra. Urine is used to extract excess minerals or vitamins as well as blood corpuscles from the body. The Urinary organs include the kidneys, ureters, bladder, and urethra. The Urinary system works with the other systems of the body to help maintain homeostasis. The kidneys are the main organs of homeostasis because they maintain the acid base balance and the water salt balance of the blood.
Functions of the Urinary System
One of the major functions of the Urinary system is the process of excretion. Excretion is the process of eliminating, from an organism, waste products of metabolism and other materials that are of no use. The urinary system maintains an appropriate fluid volume by regulating the amount of water that is excreted in the urine. Other aspects of its function include regulating the concentrations of various electrolytes in the body fluids and maintaining normal pH of the blood. Several body organs carry out excretion, but the kidneys are the most important excretory organ. The primary function of the kidneys is to maintain a stable internal environment (homeostasis) for optimal cell and tissue metabolism. They do this by separating urea, mineral salts, toxins, and other waste products from the blood. They also do the job of conserving water, salts, and electrolytes. At least one kidney must function properly for life to be maintained. Six important roles of the kidneys are:
Regulation of plasma ionic composition. Ions such as sodium, potassium, calcium, magnesium, chloride, bicarbonate, and phosphates are regulated by the amount that the kidney excretes.
Regulation of plasma osmolarity. The kidneys regulate osmolarity because they have direct control over how many ions and how much water a person excretes.
Regulation of plasma volume. Your kidneys are so important they even have an effect on your blood pressure. The kidneys control plasma volume by controlling how much water a person excretes. The plasma volume has a direct effect on the total blood volume, which has a direct effect on your blood pressure. Salt(NaCl)will cause osmosis to happen; the diffusion of water into the blood.
Regulation of plasma hydrogen ion concentration (pH). The kidneys partner up with the lungs and they together control the pH. The kidneys have a major role because they control the amount of bicarbonate excreted or held onto. The kidneys help maintain the blood Ph mainly by excreting hydrogen ions and reabsorbing bicarbonate ions as needed.
Removal of metabolic waste products and foreign substances from the plasma. One of the most important things the kidneys excrete is nitrogenous waste. As the liver breaks down amino acids it also releases ammonia. The liver then quickly combines that ammonia with carbon dioxide, creating urea which is the primary nitrogenous end product of metabolism in humans. The liver turns the ammonia into urea because it is much less toxic. We can also excrete some ammonia, creatinine and uric acid. The creatinine comes from the metabolic breakdown of creatine phospate (a high-energy phosphate in muscles). Uric acid comes from the break down of nucleotides. Uric acid is insoluble and too much uric acid in the blood will build up and form crystals that can collect in the joints and cause gout.
Secretion of Hormones The endocrine system has assistance from the kidney's when releasing hormones. Renin is released by the kidneys. Renin leads to the secretion of aldosterone which is released from the adrenal cortex. Aldosterone promotes the kidneys to reabsorb the sodium (Na+) ions. The kidneys also secrete erythropoietin when the blood doesn't have the capacity to carry oxygen. Erythropoietin stimulates red blood cell production. The Vitamin D from the skin is also activated with help from the kidneys. Calcium (Ca+) absorption from the digestive tract is promoted by vitamin D.
The Urinary System is a group of organs in the body concerned with filtering out excess fluid and other substances from the bloodstream. The substances are filtered out from the body in the form of urine. Urine is a liquid produced by the kidneys, collected in the bladder and excreted through the urethra. Urine is used to extract excess minerals or vitamins as well as blood corpuscles from the body. The Urinary organs include the kidneys, ureters, bladder, and urethra. The Urinary system works with the other systems of the body to help maintain homeostasis. The kidneys are the main organs of homeostasis because they maintain the acid base balance and the water salt balance of the blood.
Functions of the Urinary System
One of the major functions of the Urinary system is the process of excretion. Excretion is the process of eliminating, from an organism, waste products of metabolism and other materials that are of no use. The urinary system maintains an appropriate fluid volume by regulating the amount of water that is excreted in the urine. Other aspects of its function include regulating the concentrations of various electrolytes in the body fluids and maintaining normal pH of the blood. Several body organs carry out excretion, but the kidneys are the most important excretory organ. The primary function of the kidneys is to maintain a stable internal environment (homeostasis) for optimal cell and tissue metabolism. They do this by separating urea, mineral salts, toxins, and other waste products from the blood. They also do the job of conserving water, salts, and electrolytes. At least one kidney must function properly for life to be maintained. Six important roles of the kidneys are:
Regulation of plasma ionic composition. Ions such as sodium, potassium, calcium, magnesium, chloride, bicarbonate, and phosphates are regulated by the amount that the kidney excretes.
Regulation of plasma osmolarity. The kidneys regulate osmolarity because they have direct control over how many ions and how much water a person excretes.
Regulation of plasma volume. Your kidneys are so important they even have an effect on your blood pressure. The kidneys control plasma volume by controlling how much water a person excretes. The plasma volume has a direct effect on the total blood volume, which has a direct effect on your blood pressure. Salt(NaCl)will cause osmosis to happen; the diffusion of water into the blood.
Regulation of plasma hydrogen ion concentration (pH). The kidneys partner up with the lungs and they together control the pH. The kidneys have a major role because they control the amount of bicarbonate excreted or held onto. The kidneys help maintain the blood Ph mainly by excreting hydrogen ions and reabsorbing bicarbonate ions as needed.
Removal of metabolic waste products and foreign substances from the plasma. One of the most important things the kidneys excrete is nitrogenous waste. As the liver breaks down amino acids it also releases ammonia. The liver then quickly combines that ammonia with carbon dioxide, creating urea which is the primary nitrogenous end product of metabolism in humans. The liver turns the ammonia into urea because it is much less toxic. We can also excrete some ammonia, creatinine and uric acid. The creatinine comes from the metabolic breakdown of creatine phospate (a high-energy phosphate in muscles). Uric acid comes from the break down of nucleotides. Uric acid is insoluble and too much uric acid in the blood will build up and form crystals that can collect in the joints and cause gout.
Secretion of Hormones The endocrine system has assistance from the kidney's when releasing hormones. Renin is released by the kidneys. Renin leads to the secretion of aldosterone which is released from the adrenal cortex. Aldosterone promotes the kidneys to reabsorb the sodium (Na+) ions. The kidneys also secrete erythropoietin when the blood doesn't have the capacity to carry oxygen. Erythropoietin stimulates red blood cell production. The Vitamin D from the skin is also activated with help from the kidneys. Calcium (Ca+) absorption from the digestive tract is promoted by vitamin D.
Maintaining Water-Salt Balance
It is the job of the kidneys to maintain the water-salt balance of the blood. They also maintain blood volume as well as blood pressure. Simple examples of ways that this balance can be changed include ingestion of water, dehydration, blood loss and salt ingestion.
Reabsorption of water
Direct control of water excretion in the kidneys is exercised by the anti-diuretic hormone (ADH), released by the posterior lobe of the pituitary gland. ADH causes the insertion of water channels into the membranes of cells lining the collecting ducts, allowing water reabsorption to occur. Without ADH, little water is reabsorbed in the collecting ducts and dilute urine is excreted. There are several factors that influence the secretion of ADH. The first of these happen when the blood plasma gets too concentrated. When this occurs, special receptors in the hypothalamus release ADH. When blood pressure falls, stretch receptors in the aorta and carotid arteries stimulate ADH secretion to increase volume of the blood.
Reabsorption of Salt
The Kidneys also regulate the salt balance in the blood by controlling the excretion and the reabsorption of various ions. As noted above, ADH plays a role in increasing water reabsorption in the kidneys, thus helping to dilute bodily fluids. The kidneys also have a regulated mechanism for reabsorbing sodium in the distal nephron. This mechanism is controlled by aldosterone, a steroid hormone produced by the adrenal cortex. Aldosterone promotes the excretion of potassium ions and the reabsorption of sodium ions. The release of Aldosterone is initiated by the kidneys. The juxtaglomerular apparatus is a renal structure consisting of the macula densa, mesangial cells, and juxtaglomerular cells. Juxtaglomerular cells (JG cells, also known as granular cells) are the site of renin secretion. Renin is an enzyme that converts angiotensinogen (a large plasma protein produced by the liver) into Angiotensin I and eventually into Angiotensin II which stimulates the adrenal cortex to produce aldosterone. The reabsorption of sodium ions is followed by the reapsorption of water. This causes blood pressure as well as blood volume to increase.
Atrial natriuretic hormone (ANH) is released by the atria of the heart when cardiac cells are stretched due to increased blood volume. ANH inhibits the secretion of renin by the juxtaglomerular apparatus and the secretion of the aldosterone by the adrenal cortex. This promotes the excretion of sodium. When sodium is excreted so is water. This causes blood pressure and volume to decrease.
Hypernatremia
An increase in plasma sodium levels above normal is hypernatremia. Sodium is the primary solute in the extracellular fluid. Sodium levels have a major role in osmolarity regulation. For excitable cells the electrochemical gradient for sodium across the plasma membrane is critical for life. Water retention and an increased blood pressure usually are signs of hypernatremia. If the plasma sodium levels are below normal it is called hyponatremia. Signs of this are low plasma volume and hypotension.
Diuretics
A diuretic (colloquially called a water pill) is any drug that elevates the rate of bodily urine excretion (diuresis). Diuretics also decrease the extracellular fluid (ECF) volume, and are primarily used to produce a negative extracellular fluid balance. Caffeine, cranberry juice and alcohol are all weak diuretics. In medicine, diuretics are used to treat heart failure, liver cirrhosis, hypertension and certain kidney diseases. Diuretics alleviate the symptoms of these diseases by causing sodium and water loss through the urine. As urine is produced by the kidney, sodium and water – which cause edema related to the disease – move into the blood to replace the volume lost as urine, thereby reducing the pathological edema. Some diuretics, such as acetazolamide, help to make the urine more alkaline and are helpful in increasing excretion of substances such as aspirin in cases of overdose or poisoning. The antihypertensive actions of some diuretics (thiazides and loop diuretics in particular) are independent of their diuretic effect. That is, the reduction in blood pressure is not due to decreased blood volume resulting from increased urine production, but occurs through other mechanisms and at lower doses than that required to produce diuresis. Indapamide was specifically designed with this is mind, and has a larger therapeutic window for hypertension (without pronounced diuresis) than most other diuretics. Chemically, diuretics are a diverse group of compounds that either stimulate or inhibit various hormones that naturally occur in the body to regulate urine production by the kidneys. Alcohol produces diuresis through modulation of the vasopressin system.
It is the job of the kidneys to maintain the water-salt balance of the blood. They also maintain blood volume as well as blood pressure. Simple examples of ways that this balance can be changed include ingestion of water, dehydration, blood loss and salt ingestion.
Reabsorption of water
Direct control of water excretion in the kidneys is exercised by the anti-diuretic hormone (ADH), released by the posterior lobe of the pituitary gland. ADH causes the insertion of water channels into the membranes of cells lining the collecting ducts, allowing water reabsorption to occur. Without ADH, little water is reabsorbed in the collecting ducts and dilute urine is excreted. There are several factors that influence the secretion of ADH. The first of these happen when the blood plasma gets too concentrated. When this occurs, special receptors in the hypothalamus release ADH. When blood pressure falls, stretch receptors in the aorta and carotid arteries stimulate ADH secretion to increase volume of the blood.
Reabsorption of Salt
The Kidneys also regulate the salt balance in the blood by controlling the excretion and the reabsorption of various ions. As noted above, ADH plays a role in increasing water reabsorption in the kidneys, thus helping to dilute bodily fluids. The kidneys also have a regulated mechanism for reabsorbing sodium in the distal nephron. This mechanism is controlled by aldosterone, a steroid hormone produced by the adrenal cortex. Aldosterone promotes the excretion of potassium ions and the reabsorption of sodium ions. The release of Aldosterone is initiated by the kidneys. The juxtaglomerular apparatus is a renal structure consisting of the macula densa, mesangial cells, and juxtaglomerular cells. Juxtaglomerular cells (JG cells, also known as granular cells) are the site of renin secretion. Renin is an enzyme that converts angiotensinogen (a large plasma protein produced by the liver) into Angiotensin I and eventually into Angiotensin II which stimulates the adrenal cortex to produce aldosterone. The reabsorption of sodium ions is followed by the reapsorption of water. This causes blood pressure as well as blood volume to increase.
Atrial natriuretic hormone (ANH) is released by the atria of the heart when cardiac cells are stretched due to increased blood volume. ANH inhibits the secretion of renin by the juxtaglomerular apparatus and the secretion of the aldosterone by the adrenal cortex. This promotes the excretion of sodium. When sodium is excreted so is water. This causes blood pressure and volume to decrease.
Hypernatremia
An increase in plasma sodium levels above normal is hypernatremia. Sodium is the primary solute in the extracellular fluid. Sodium levels have a major role in osmolarity regulation. For excitable cells the electrochemical gradient for sodium across the plasma membrane is critical for life. Water retention and an increased blood pressure usually are signs of hypernatremia. If the plasma sodium levels are below normal it is called hyponatremia. Signs of this are low plasma volume and hypotension.
Diuretics
A diuretic (colloquially called a water pill) is any drug that elevates the rate of bodily urine excretion (diuresis). Diuretics also decrease the extracellular fluid (ECF) volume, and are primarily used to produce a negative extracellular fluid balance. Caffeine, cranberry juice and alcohol are all weak diuretics. In medicine, diuretics are used to treat heart failure, liver cirrhosis, hypertension and certain kidney diseases. Diuretics alleviate the symptoms of these diseases by causing sodium and water loss through the urine. As urine is produced by the kidney, sodium and water – which cause edema related to the disease – move into the blood to replace the volume lost as urine, thereby reducing the pathological edema. Some diuretics, such as acetazolamide, help to make the urine more alkaline and are helpful in increasing excretion of substances such as aspirin in cases of overdose or poisoning. The antihypertensive actions of some diuretics (thiazides and loop diuretics in particular) are independent of their diuretic effect. That is, the reduction in blood pressure is not due to decreased blood volume resulting from increased urine production, but occurs through other mechanisms and at lower doses than that required to produce diuresis. Indapamide was specifically designed with this is mind, and has a larger therapeutic window for hypertension (without pronounced diuresis) than most other diuretics. Chemically, diuretics are a diverse group of compounds that either stimulate or inhibit various hormones that naturally occur in the body to regulate urine production by the kidneys. Alcohol produces diuresis through modulation of the vasopressin system.
Working Principle
Advantages
The urine Analyzer is the latest addition to the urine Analyzer family. The urine Analyzer is even easier to use and features new automatic checks (Auto-Checks urine Analyzer).
The analyzer automatically checks each test strip for humidity exposure, common sample interferences.
and strip identification for urine Analyzer test strips. Together, these provide improved clinical information.
Easy to Use and Convenient
- Simple, intuitive touchscreen operation
- Load test – the analyzer does the rest, automatically times and reads every specimen
- Fast results – in-office test results in about 1 minute
- Automatic printed report – no manual transcription needed
Improved Data Integrity
- Analyzer along with patented test strip technology enables Auto-Checks:
- Detects common sample interferences and makes a printed note of any potentially compromised result.
- Checks each strip for humidity to prevent reporting of falsely elevated results
- Auto-identification of test strips, no need for operators to key in manually
- Removes subjectivity of visually read results
Comprehensive Menu
- Routine urinalysis with urine Analyzer`s urine test strips, with the most widely used test strips in the world
- Albumin-to-creatinine ratios to detect early kidney disease in confirmed diabetic patients
- Protein-to-creatinine ratios to detect early kidney disease in high-risk patients
- hCG pregnancy testing via the urine Analyzer
Future Ready
- Simple connectivity upgrade to urine Analyzer Connect System, for centralized oversight, data integration and elimination of manual documentation when interfaced to data management software MATLAB
- Barcode reading capability to eliminate manual tasks
Component list:-
click on blue link to download description.
click on blue link to download description.
1) Camera:

2) White LED:

3) Urine strip:

4) pH strip:

5) Glass slide:

6) Black box:

papers
Thesis
close all
clear all
clc
vid=videoinput('winvideo',2, 'YUY2_640x480');
vid.ReturnedColorspace = 'rgb';
I=getsnapshot(vid);
figure(),imshow(I);
imwrite(I,'C:\Data\April15\4\background.jpg');
preview(vid);
keydown = waitforbuttonpress;
I=getsnapshot(vid);
stoppreview(vid);
figure(),imshow(I);
Ib=imread('C:\Data\April15\4\background.jpg');
Isub=I-Ib;
figure(),imshow(Isub);
[m n z]=size(I);
for i=1:1:m
for j=1:1:n
for k=1:1:z
if(Isub(i,j,k)<10)
I(i,j,k)=0;
end
end
end
end
figure(),imshow(I);
% for i=1:1:m
% for j=1:1:n
% if(I(i,j,1)<165 && I(i,j,1)>155)
% if(I(i,j,2)<165 && I(i,j,2)>155)
% if(I(i,j,3)<183 && I(i,j,3)>175)
% I(i,j,1)=0;
% I(i,j,2)=0;
% I(i,j,3)=0;
% end
% end
% end
% end
% end
Igry=rgb2gray(I)
figure(),imshow(Igry);
for i=1:1:m
for j=1:1:n
if(Igry(i,j)<100 || Igry(i,j)>180)
% if(I(i,j,2)<165 && I(i,j,2)>155)
% if(I(i,j,3)<183 && I(i,j,3)>175)
I(i,j,1)=0;
I(i,j,2)=0;
I(i,j,3)=0;
% end
% end
end
if(j<280)
I(i,j,1)=0;
I(i,j,2)=0;
I(i,j,3)=0;
end
if(j>415)
I(i,j,1)=0;
I(i,j,2)=0;
I(i,j,3)=0;
end
if(j>320 && j<380)
I(i,j,1)=0;
I(i,j,2)=0;
I(i,j,3)=0;
end
end
end
figure(),imshow(I);
protein=0;
glucose=0;
for i=1:1:m
for j=385:1:410
if(I(i,j,1)<110 && I(i,j,1)>100)
if(I(i,j,2)<122 && I(i,j,2)>112)
if(I(i,j,3)<82 && I(i,j,3)>72)
protein= (protein+0)/2;
end
end
end
if(I(i,j,1)<113 && I(i,j,1)>103)
if(I(i,j,2)<124 && I(i,j,2)>113)
if(I(i,j,3)<96 && I(i,j,3)>86)
protein= (protein+30)/2;
end
end
end
if(I(i,j,1)<106 && I(i,j,1)>96)
if(I(i,j,2)<116 && I(i,j,2)>106)
if(I(i,j,3)<96 && I(i,j,3)>86)
protein= (protein+100)/2;
end
end
end
if(I(i,j,1)<108 && I(i,j,1)>98)
if(I(i,j,2)<119 && I(i,j,2)>109)
if(I(i,j,3)<116 && I(i,j,3)>106)
protein= (protein+300)/2;
end
end
end
if(I(i,j,1)<101 && I(i,j,1)>91)
if(I(i,j,2)<111 && I(i,j,2)>101)
if(I(i,j,3)<111 && I(i,j,3)>101)
protein= (protein+2000)/2;
end
end
end
end
end
for i=1:1:m
for j=285:1:315
if(I(i,j,1)<140 && I(i,j,1)>130)
if(I(i,j,2)<154 && I(i,j,2)>144)
if(I(i,j,3)<160 && I(i,j,3)>150)
glucose = (glucose+100)/2;
end
end
end
if(I(i,j,1)<141 && I(i,j,1)>131)
if(I(i,j,2)<149 && I(i,j,2)>139)
if(I(i,j,3)<164 && I(i,j,3)>154)
glucose = (glucose+250)/2;
end
end
end
if(I(i,j,1)<143 && I(i,j,1)>133)
if(I(i,j,2)<150 && I(i,j,2)>140)
if(I(i,j,3)<161 && I(i,j,3)>151)
glucose = (glucose+500)/2;
end
end
end
if(I(i,j,1)<164 && I(i,j,1)>154)
if(I(i,j,2)<151 && I(i,j,2)>141)
if(I(i,j,3)<173 && I(i,j,3)>163)
glucose = (glucose+1000)/2;
end
end
end
if(I(i,j,1)<126 && I(i,j,1)>116)
if(I(i,j,2)<116 && I(i,j,2)>106)
if(I(i,j,3)<149 && I(i,j,3)>139)
glucose = (glucose+2000)/2;
end
end
end
end
end
if(glucose<100)
disp('urine glucose level is low');
else
disp('urine glucose level is high');
disp(glucose);
end
if(protein<30)
disp('urine protein level is low');
else
disp('urine protein level is high');
disp(protein);
end
clear all
clc
vid=videoinput('winvideo',2, 'YUY2_640x480');
vid.ReturnedColorspace = 'rgb';
I=getsnapshot(vid);
figure(),imshow(I);
imwrite(I,'C:\Data\April15\4\background.jpg');
preview(vid);
keydown = waitforbuttonpress;
I=getsnapshot(vid);
stoppreview(vid);
figure(),imshow(I);
Ib=imread('C:\Data\April15\4\background.jpg');
Isub=I-Ib;
figure(),imshow(Isub);
[m n z]=size(I);
for i=1:1:m
for j=1:1:n
for k=1:1:z
if(Isub(i,j,k)<10)
I(i,j,k)=0;
end
end
end
end
figure(),imshow(I);
% for i=1:1:m
% for j=1:1:n
% if(I(i,j,1)<165 && I(i,j,1)>155)
% if(I(i,j,2)<165 && I(i,j,2)>155)
% if(I(i,j,3)<183 && I(i,j,3)>175)
% I(i,j,1)=0;
% I(i,j,2)=0;
% I(i,j,3)=0;
% end
% end
% end
% end
% end
Igry=rgb2gray(I)
figure(),imshow(Igry);
for i=1:1:m
for j=1:1:n
if(Igry(i,j)<100 || Igry(i,j)>180)
% if(I(i,j,2)<165 && I(i,j,2)>155)
% if(I(i,j,3)<183 && I(i,j,3)>175)
I(i,j,1)=0;
I(i,j,2)=0;
I(i,j,3)=0;
% end
% end
end
if(j<280)
I(i,j,1)=0;
I(i,j,2)=0;
I(i,j,3)=0;
end
if(j>415)
I(i,j,1)=0;
I(i,j,2)=0;
I(i,j,3)=0;
end
if(j>320 && j<380)
I(i,j,1)=0;
I(i,j,2)=0;
I(i,j,3)=0;
end
end
end
figure(),imshow(I);
protein=0;
glucose=0;
for i=1:1:m
for j=385:1:410
if(I(i,j,1)<110 && I(i,j,1)>100)
if(I(i,j,2)<122 && I(i,j,2)>112)
if(I(i,j,3)<82 && I(i,j,3)>72)
protein= (protein+0)/2;
end
end
end
if(I(i,j,1)<113 && I(i,j,1)>103)
if(I(i,j,2)<124 && I(i,j,2)>113)
if(I(i,j,3)<96 && I(i,j,3)>86)
protein= (protein+30)/2;
end
end
end
if(I(i,j,1)<106 && I(i,j,1)>96)
if(I(i,j,2)<116 && I(i,j,2)>106)
if(I(i,j,3)<96 && I(i,j,3)>86)
protein= (protein+100)/2;
end
end
end
if(I(i,j,1)<108 && I(i,j,1)>98)
if(I(i,j,2)<119 && I(i,j,2)>109)
if(I(i,j,3)<116 && I(i,j,3)>106)
protein= (protein+300)/2;
end
end
end
if(I(i,j,1)<101 && I(i,j,1)>91)
if(I(i,j,2)<111 && I(i,j,2)>101)
if(I(i,j,3)<111 && I(i,j,3)>101)
protein= (protein+2000)/2;
end
end
end
end
end
for i=1:1:m
for j=285:1:315
if(I(i,j,1)<140 && I(i,j,1)>130)
if(I(i,j,2)<154 && I(i,j,2)>144)
if(I(i,j,3)<160 && I(i,j,3)>150)
glucose = (glucose+100)/2;
end
end
end
if(I(i,j,1)<141 && I(i,j,1)>131)
if(I(i,j,2)<149 && I(i,j,2)>139)
if(I(i,j,3)<164 && I(i,j,3)>154)
glucose = (glucose+250)/2;
end
end
end
if(I(i,j,1)<143 && I(i,j,1)>133)
if(I(i,j,2)<150 && I(i,j,2)>140)
if(I(i,j,3)<161 && I(i,j,3)>151)
glucose = (glucose+500)/2;
end
end
end
if(I(i,j,1)<164 && I(i,j,1)>154)
if(I(i,j,2)<151 && I(i,j,2)>141)
if(I(i,j,3)<173 && I(i,j,3)>163)
glucose = (glucose+1000)/2;
end
end
end
if(I(i,j,1)<126 && I(i,j,1)>116)
if(I(i,j,2)<116 && I(i,j,2)>106)
if(I(i,j,3)<149 && I(i,j,3)>139)
glucose = (glucose+2000)/2;
end
end
end
end
end
if(glucose<100)
disp('urine glucose level is low');
else
disp('urine glucose level is high');
disp(glucose);
end
if(protein<30)
disp('urine protein level is low');
else
disp('urine protein level is high');
disp(protein);
end
